Routine screening is recommended for individuals aged 13 to 64 at least once as part of standard preventive healthcare. At Rap-It-Up, we believe that knowing your status is the ultimate flex. We are here to break down the stigma surrounding HIV and provide you with the real, no-nonsense facts about sexual health. Protect yourself, protect your partner, and empower your community.
The Role of Routine Screening in Preventive Healthcare
Historically, sexual health screenings carried an unwarranted weight of anxiety. Patients often viewed the process as an exceptional event rather than a standard medical procedure. To counter this, community health centers integrated HIV testing directly into primary care visits. When a primary care physician introduces the topic alongside blood pressure and cholesterol checks, it strips away the moral panic that historically surrounded the virus.
This shift normalizes the conversation—transforming a dreaded appointment into a standard health check.
By treating the screening as a routine vital sign, providers remove the stigma associated with requesting a test. The measured impact of this approach is clear. Patients report feeling significantly less apprehension when the test is presented as a proven, standard component of their overall health maintenance. You can review the CDC guidelines on HIV testing to understand how these recommendations shape clinical practice.
Pre-Test Preparation and Risk Assessment
Walking into a clinic for the first time requires preparation. Before any physical test occurs, patients must complete intake forms and provide informed consent. The physical environment of the clinic plays a crucial role in this stage. Moving away from cold, sterile waiting rooms to more private, comfortable consultation spaces encourages honesty.
Clinic coordinators initially used a standard 4-page clinical intake questionnaire, but found it caused visible anxiety in younger patients. They transitioned to a conversational, provider-led risk assessment. During outreach, I frequently observe how this shift transforms the patient experience.
Intake and risk assessment conversations typically take 5 to 15 minutes. Providers use this time to discuss sexual health history without judgment. The outcome is a collaborative decision on the most appropriate type of test for the patient's specific situation.
Field Note: First-Time HIV Screening Preparation Checklist
- Bring a valid photo ID if using insurance or confidential testing (not required for anonymous testing).
- Have a general timeline of recent sexual partners or potential exposure events over the last 3 to 6 months.
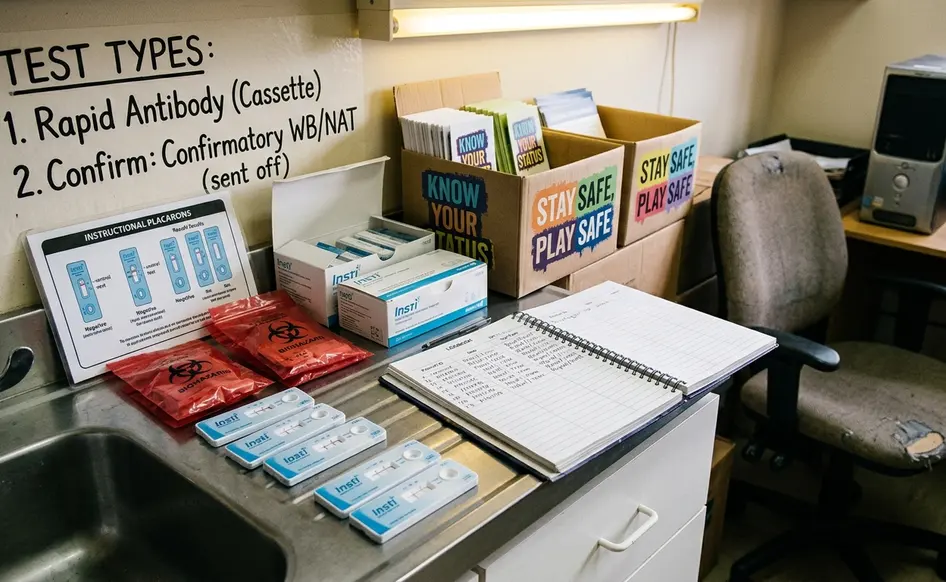
Diagnostic Modalities: Types of HIV Tests Administered
Understanding the science behind the screening alleviates fear of the unknown. Clinics use specific diagnostic tools based on the timing of potential exposure and available laboratory infrastructure. The science of detection has evolved rapidly over the last two decades, moving from tests that required weeks of waiting to highly refined, rapid technology.
Rapid antibody tests use oral fluid or a finger prick drop of roughly 50 microliters. These tests look for the body's immune response to the virus. Antigen/Antibody lab tests require a venous draw of 4 to 5 milliliters of blood. This modality detects both antibodies and the p24 antigen, offering a more comprehensive analysis.
Nucleic Acid Tests (NAT) are generally reserved for high-risk exposures within the last 7 to 14 days due to higher cost and complexity.
Selecting the optimal test depends entirely on the patient's recent sexual history.
The Step-by-Step Clinical Procedure
Fear of needles remains a significant barrier to preventive care. Recognizing this community need, certified testing centers adopted less invasive collection methods wherever clinically appropriate. The physical process is swift and highly regulated. By demystifying the exact physical steps, clinics empower patients to take control of their health.
Oral swabs require swabbing the upper and lower gums once each, taking about 10 seconds.
For blood-based rapid tests, finger pricks use a single-use, auto-retracting lancet, typically 21 to 23 gauge, to minimize discomfort. The provider cleans the site, deploys the lancet, and collects the sample in moments. A venous blood draw involves applying a tourniquet, sanitizing the arm, and collecting vials for laboratory analysis. Patients consistently report that the actual procedure is far less intimidating than their initial expectations.
Navigating Patient Privacy and Confidentiality
Community feedback indicates a persistent concern regarding who has access to sexual health records. The systemic challenge lies in balancing necessary medical documentation with the patient's right to privacy. Navigating the healthcare system requires an understanding of your rights, as privacy is not just a courtesy; it is a legal mandate.
The pathway forward involves clear communication about the difference between confidential and anonymous testing. Confidential testing ties results to medical records but remains protected by HIPAA regulations. Anonymous testing sites generate a unique alphanumeric identifier, such as a 9-digit code, instead of using a legal name to ensure the result cannot be linked to a standard electronic health record.
The availability of truly anonymous testing versus confidential testing depends heavily on state laws and specific clinic funding structures. Ongoing, multi-year partnerships between advocacy groups and health departments continue to expand access to these protected services.
Important: Guaranteed privacy protocols mean your health data remains secure, but you must ask your specific clinic how they classify their records before beginning the intake process.
Understanding Results and Window Period Limitations
Interpreting the outcome of a screening requires an understanding of biological timelines. The human body takes time to mount a detectable response to any pathogen. This biological reality dictates the testing schedule. The 'window period' is the time between potential exposure and when a test can accurately detect the virus.
Assuming a rapid oral test will detect an exposure that occurred 48 hours prior is a dangerous misconception.
Window periods vary significantly by modality: 18 to 90 days for rapid antibody tests, 18 to 45 days for lab-based antigen/antibody tests, and 10 to 33 days for NATs.
One catch: a negative result on a rapid test administered just three weeks after a potential exposure cannot definitively rule out transmission, necessitating a follow-up test at the 90-day mark.
Preliminary positive results always require secondary confirmatory laboratory testing. While clinical protocols standardize the testing process, individual clinic resources dictate the specific modalities available.
Bottom Line: A single test provides a snapshot of your health at a specific point in time, making routine screening the most effective strategy for long-term wellness.
Citations
- Centers for Disease Control and Prevention. HIV Testing Guidelines.
- Clinical data regarding window periods and diagnostic modalities sourced from standard epidemiological reference materials.

Your Thoughts
The conversation starts with you.
Your Comment