
Defining Comprehensive Sexual Health
Young adults often encounter sexual health education framed entirely around fear. Curriculum developers debated whether to lead our recent multi-year initiative with local STI transmission rates. They opted to center five foundational pillars first to establish a proactive mindset. These pillars include barrier methods, routine screening, communication, preventive medication, and emergency protocols.
This approach treats sexual health as a routine part of overall wellness rather than a crisis waiting to happen. Knowing your status and having a plan is the ultimate flex. It empowers individuals to protect themselves and their partners without the heavy burden of stigma.
1. Consistent and Correct Barrier Method Use
Educators shifted the focus of barrier method instruction from basic application mechanics to material science. Understanding how environmental factors and chemical interactions degrade structural integrity changes how people use these tools.
Latex degradation accelerates rapidly when exposed to oil-based products like petroleum jelly or mineral oil. We teach people to pair latex exclusively with water-based or silicone-based lubricants. For individuals with latex sensitivities, polyurethane and polyisoprene alternatives provide reliable protection.
Field Note: Store barrier methods away from extreme heat or friction to maintain their material integrity.
2. Proactive STI and HIV Screening Protocols
Community feedback indicates that a universal annual testing date rarely aligns with actual lived experiences. The advisory board moved away from recommending a single yearly visit. They structured the protocol around individual partner frequency and specific exposure events to reduce false negatives.
Testing frequency recommendations shift from annually to every three months based on two factors—the number of concurrent partners and local transmission rates.

Understanding window periods is critical. There is an 18 to 90-day window period for 4th generation HIV antigen/antibody tests. Gonorrhea has a 2 to 6-day incubation period before accurate detection via nucleic acid amplification testing. Relying on rapid HIV tests too early in the window period results in a false negative due to insufficient antibody development.
3. Transparent Partner Communication Frameworks
Our program data showed that providing rigid, word-for-word disclosure scripts for young adults simply did not work. Participants dropped them after feedback indicated they felt unnatural. The framework was subsequently redesigned into modular talking points.
While self-reported participant surveys suggest high engagement with these new modules, the most proven strategy involves initiating dialogue in a neutral environment at least 24 hours prior to anticipated intimacy. This removes the immediate pressure of the bedroom. It allows both partners to establish clear boundaries and mutual consent regarding barrier usage. Direct, compassionate dialogue helps overcome the stigma associated with discussing sexual health history.
4. Pre-Exposure Prophylaxis (PrEP) and Vaccinations
To address adherence barriers such as pill fatigue among young adults, the clinical outreach team decided to equally weight daily oral PrEP and long-acting injectable options in the educational materials.
PrEP injectables are administered every two months following an initial initiation phase. This significantly reduces the daily burden of acquiring HIV protection.
Vaccinations play an equally vital role in long-term health. The HPV vaccine series is administered on a 0, 2, and 6-month schedule. This prevents certain strains of the virus associated with long-term health complications. Consulting with healthcare providers helps determine eligibility and access programs for these preventive medications.
5. Emergency Contraception and Post-Exposure Protocols (PEP)
When designing the emergency protocol section, health communicators prioritized the strict timeline over the pharmacological mechanism of action to drive immediate clinical action. There is a 72-hour maximum window to initiate Post-Exposure Prophylaxis (PEP) after a potential HIV exposure.
Once initiated, a 28-day continuous daily regimen is required for PEP efficacy. Locating urgent care or community health clinics equipped to provide time-sensitive interventions is a necessary step when primary barrier methods fail.
Important: PEP is strictly for isolated emergency exposures and cannot be prescribed as a substitute for ongoing PrEP regimens.
Scope and Limitations of Prevention Strategies
No single prevention method offers absolute certainty against all risks. The team adopted the 'Swiss Cheese Model' from occupational safety to visually demonstrate to community advocates how combining imperfect prevention methods creates a strong defense.
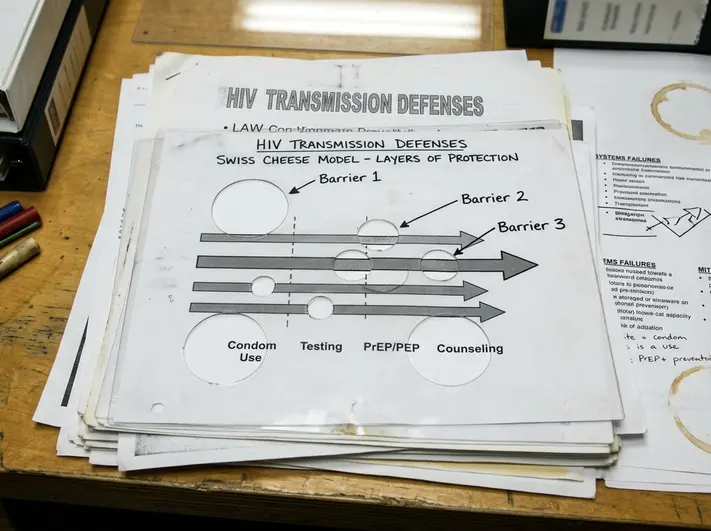
Layering barrier methods with PrEP and a 3 to 6-month screening cadence covers individual method vulnerabilities. Recognizing systemic barriers to healthcare access helps identify community resources that bridge these gaps. You can review the official prevention guidelines to understand how these layers work together in practice.
Pre-Clinic Visit Preparation Checklist
Bottom Line: Arriving prepared maximizes the value of your clinical consultation.
- List of current medications and supplements to check for PrEP contraindications
- Dates of last known potential exposures to calculate testing window periods
- Record of previous vaccinations (e.g., HPV, Hepatitis B)
- Specific questions regarding barrier method alternatives or lubricant compatibility
Citations
Data regarding window periods, vaccination schedules, and material degradation profiles are drawn directly from the foundational pillars established by the curriculum advisory board and clinical outreach teams.


Your Thoughts
The conversation starts with you.
Your Comment